A groundbreaking study from the University of Illinois, Chicago, published in the American Journal of Psychiatry, reveals a potential link between suicidal thoughts and specific menstrual cycle phases, particularly for women with premenstrual dysphoric disorder (PMDD). Tracking 119 women with mental health disorders, the research found heightened suicide risk in the days around menstruation, challenging prior assumptions. Significantly, this risk isn’t exclusive to PMDD, emphasizing broader implications. The study’s daily mood tracking, a departure from past limitations, provides a comprehensive understanding and calls for increased awareness and tailored interventions acknowledging the cyclical nature of mental health challenges.
Spread the love
In a groundbreaking study published in the American Journal of Psychiatry, researchers at the University of Illinois, Chicago have shed light on a potential link between suicidal thoughts and specific phases of the menstrual cycle, particularly for women diagnosed with premenstrual dysphoric disorder (PMDD). The study, the first of its kind to explore suicide risk through daily mood tracking, unveils intriguing findings that challenge historical limitations in research on the menstrual cycle and suicide.
The Study Design
The research focused on 119 women diagnosed with mental health disorders, substance use disorder, or eating disorders. These participants were closely monitored throughout an entire menstrual cycle, with daily tracking of mood and suicidal ideation. The emphasis on daily mood tracking sets this study apart from previous research, providing a comprehensive understanding of the fluctuations in mental health throughout the menstrual cycle.
Key Findings
Temporal Correlation with Menstrual Cycle
The study found a notable connection between suicidal thoughts, planning, and attempts and specific times during the menstrual cycle. Interestingly, these risk factors were most prevalent in the days preceding and following menstruation. This temporal correlation challenges conventional wisdom and underscores the need for a nuanced understanding of the menstrual cycle’s impact on mental health.
Broad Applicability Beyond PMDD
Contrary to prior assumptions, the research reveals that the heightened risk of suicide is not exclusive to individuals with premenstrual dysphoric disorder. Instead, the association with the menstrual cycle was observed across various mental health diagnoses, emphasizing the broader implications of the findings.
Significance of the Study
The significance of this study lies in its departure from the historical limitations imposed by small, cross-sectional samples in research on the menstrual cycle and suicide. By employing a large transdiagnostic sample of females with suicidal ideation, the study provides a pioneering contribution to understanding the intricate pathways through which the menstrual cycle influences acute suicide risk.
According to the researchers, “Research on the menstrual cycle and suicide has been limited historically by small, cross-sectional samples. This study provides the first evidence that measuring day-to-day correlates of suicidality in a large transdiagnostic sample of females with suicidal ideation can contribute to understanding the pathways by which the menstrual cycle influences acute suicide risk.
As we navigate the complex intersection of mental health and the menstrual cycle, this study serves as a beacon, guiding researchers and clinicians toward a more comprehensive understanding of the factors influencing suicide risk. The findings not only underscore the need for further exploration but also call for increased awareness and tailored interventions that consider the cyclical nature of mental health challenges faced by individuals.
📝🎤 Hold onto your seats, it's Meghna Sakshi—a master storyteller who can turn any info into captivating tales with a flick of the pen. As an anchor, I've wrangled even the trickiest topics into submission, and as a content maestro, my words have a habit of sticking around. When I'm not chasing stories, I'm probably chasing down a cup of coffee or the next great adventure. But there's more to it: I aim to shed light on crucial women-centric issues, spreading awareness and empowerment through my blogs. So buckle up, because with me, even the stories get a dose of excitement! 🚀📰
We are speaking so much about women’s health on Infano, – physical, mental, and sexual. But while giving relationship tips for women, we cannot ignore the health of male partners because the balance for any good sound and healthy relationship requires both partners to be in sync- both physically and mentally.
However, most men are shy to talk about their health especially when it comes to sexual health. A lot of cultural upbringing also surrounds these inhibitions because so much toxic masculinity abounds and sexualized terms like namard, napunsak, impotent, khada nahi hota kya, are some slurs used often for bullying each other that men often don’t want to discuss this for fear of mean ridiculed that he is not “man enough”.
Sexual performance anxiety in bed is a real thing for most men. Though sex is just another hormone- bodily function for reproduction, it is also a pleasurable activity. It is also an activity that bonds two people. So sexual health and well-being are of utmost importance if one is sexually active and wishes to enjoy it.
Relationship tips for women: Learn about the ‘Male Orgasm’
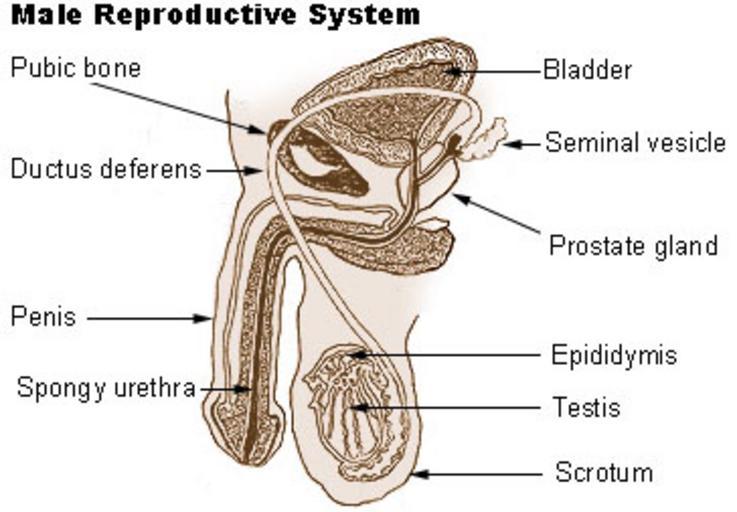
The male reproductive system
The male orgasm is the third of four distinct phases comprising ejaculation: arousal, plateau, orgasm, and resolution/refraction, although not all men ejaculate during an orgasm. Male orgasm results from sexual activity (physical sensation) and arousal (cognitive awareness). It involves multiple hormones, organs, and nerve pathways. Testosterone, a hormone produced in the testicles, plays a central role in this process by enhancing sexual desire (libido) that leads to arousal, erection, and ultimately, orgasm. Also involved are contractions of the muscles of the penis, anus, and perineum which ultimately propel semen from the body. During orgasm, the reward center of the brain is flooded with neurochemicals, inciting the intense emotional response associated with an orgasm. When any of these aspects are affected by physical or emotional issues, the individual may be unable to achieve a normal orgasm.
According to an article by the Harvard Medical School, optimal sexual health for people with penises includes sexual desire (libido) and the ability to get and sustain an erection (erectile function). Male sexual health also covers the prevention and treatment of sexually transmitted diseases and the assessment and treatment of male infertility.
While these conditions do not pose serious medical risks, they can cause stress and create problems in your sex life and personal relationships. Physical health does affect the desire for sex and the ability to have sex, but mental health and emotional factors also play important roles.
What are the common male sexual problems?
What is Erectile dysfunction (ED)
This is the inability to get an erection or to keep it firm enough or maintain it long enough for satisfying sexual activity. Many things can cause ED, including stress, depression, relationship issues, abnormally low testosterone, damage from urological surgery, and even cholesterol-clogged arteries. In fact, it is often an early warning sign for heart disease. Patients suffering from erectile dysfunction should first be evaluated for any underlying physical and psychological conditions. If treatment of the underlying conditions doesn’t help, medication and assistive devices, such as pumps, can be prescribed. ED can be treated with pills, injections into the penis, or devices.
What are the types of ejaculation difficulties?
Premature ejaculation
This is the inability to delay ejaculation for more than one minute after penetration. The problem might occur during sex with a partner or even during masturbation. Some men might experience natural variable premature ejaculation, which includes periods of rapid ejaculation as well as periods of normal ejaculation. But this does not qualify diagnostic criteria. The average time from the beginning of intercourse to ejaculation is about five minutes. But lifelong premature ejaculation occurs all or nearly all of the time beginning with your first sexual encounters. Premature ejaculation is a common and treatable problem. Physical and psychological factors can cause premature ejaculation. Medications, counseling and sexual techniques that delay ejaculation — or a combination of these — can help treat this.
Delayed ejaculation
Delayed ejaculation (DE) or “impaired ejaculation,” occurs when it takes a long time for a man to ejaculate. In some cases, ejaculation cannot be achieved at all. While some men experience DE from time to time, but for others, it may be a lifelong problem. When people with penises need 30 minutes of sexual stimulation to reach orgasm and ejaculate.
This is a common medical condition. Delayed ejaculation appears to be caused by an underlying problem that might need treatment. A medical exam, blood test, and urine tests (urinalysis) may be conducted. Delayed ejaculation treatment depends on the underlying cause, but it might include taking medication or making changes to medications you currently take, undergoing psychological counseling, or addressing alcohol or illegal drug use.
Anorgasmia or inability to experience orgasm upon ejaculation
Anorgasmia is a condition that can affect both sexes. Anorgasmia in people with penises often occurs along with delayed ejaculation and should not be confused with erectile dysfunction or low libido, although these conditions may co-exist. Causes include physiological problems present at birth to side effects from surgery or medications to psychological issues. Treatment is determined once the cause is determined.
Blood tests, biothesiometry, penile sympathetic skin response, and sacral reflex arc testing are some of the medical tests that may be required along with a physical exam and a psychological evaluation. Some medications may also cause this. Treatment may include reevaluating medical prescriptions, psychotherapy, sex therapy, digital prostate massage, or hormone replacement therapy.
From identifying the problem, determining its underlying cause, and getting the right treatment, all of these conditions are mostly treatable. However, the first step is to identify and accept that a problem exists and giving your partner a safe, non-judgemental space to talk about it and the necessary support and medical attention.
Tasneem Akbari Kutubuddin has done her masters in Journalism & Communication and has worked as a senior journalist, editor and columnist for leading publications like The Logical Indian, Deccan Chronicle, Worldwide Media Corporation, The Bridge and Provoke.
With Infano, she hopes to create more awareness about women’s health issues. Suffering with Fibromyalgia, a chronic pain condition, she has also been advocating for its awareness through media.